New report reveals need for more humane, personalized approach in European Region’s long-term institutions for adults with intellectual and psychosocial disabilities
Извор: Светска здравствена организација – 06.06.2018
 WHO
WHO
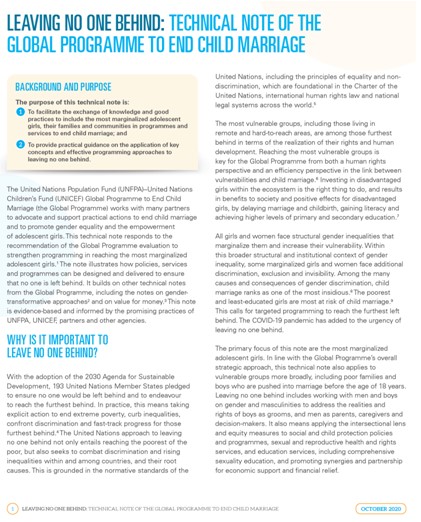
WHO/Europe has released a new report entitled “Mental health, human rights and standards of care”. It assesses the quality of institutional care for adults with psychosocial and intellectual disabilities in the WHO European Region.
A total of 75 institutions across 24 countries in the Region and Kosovo (in accordance with United Nations Security Council resolution 1244 [1999]) were assessed using the WHO QualityRights Toolkit. Out of all the quality ratings made, only 25% showed compliance with international standards, meaning that long-term institutional care in the Region has significant room for improvement.
“These assessments provide a window into the state of institutional care in Europe,” said Dr Zsuzsanna Jakab, WHO Regional Director for Europe. “We should take the findings as an important wake-up call that more should and must be done to guarantee that human rights are fully respected in institutional care, with the ultimate goal of moving towards different and better models of care for mental health.”
The assessments used the WHO QualityRights Toolkit to collect and report data on standards related to 5 themes from the United Nations Convention on the Rights of Persons with Disabilities (CRPD):
- the right to an adequate standard of living (Article 28);
- the right to enjoyment of the highest attainable standard of physical and mental health (Article 25);
- the right to exercise legal capacity and the right to personal liberty and security of person (Articles 12 and 14);
- freedom from torture or cruel, inhuman or degrading treatment or punishment and from exploitation, violence and abuse (Articles 15 and 16); and
- the right to live independently and be included in the community (Article 19).
Here, Dr Daniel Chisholm, Programme Manager for Mental Health at WHO/Europe and project lead for the report, explains what the results mean for the Region and how countries can make positive changes to institutional care, even with limited resources.
What prompted the mental health programme to take a closer look at the topic of mental health and human rights and to push for this assessment?
This is the latest phase of a project that actually started several years ago when some reports coming out of countries were brought to the attention of the Regional Director. These reports indicated very serious breaches and violations of human rights and failings of standards of care within long-term institutions.
The first phase of the WHO/Europe response was descriptive, focused on understanding more about how many facilities there are, who lives in them, their characteristics and so forth. Now we have moved into the second and more substantive phase, looking at what’s going on behind the closed doors of these institutions, in terms of quality of care provided and the extent to which human rights are being protected – or not protected, as the case may be.
What did the country teams find when they conducted their assessments?
The assessments revealed a number of overarching concerns. First, there is a lack of awareness about mental health and human rights in the first place, even among staff – an underappreciation of the basic rights of the individuals living in these institutions. Second, there is a lack of a humane, or personalized, approach. The idea of an individualized plan of care is embedded within the CRPD. It’s an important concept in mental health, where even if individuals have substantial impairments, you can still develop an individualized plan for improvement or recovery. And that is often missing in these places. In other words, people have no kind of hope and no idea about the journey they’re on; instead, it seems like an endless tunnel.
Another concerning thing coming out of a number of these reports is that there is little or nothing for people to do in these institutions, and people are actually not allowed to do basic things that we all take for granted. It doesn’t matter if you’re living in your own home or in a long-term institution – you should be able to pick up a telephone and call your family, or you should be able to watch television or find a quiet area to read a book. The simple pleasures in life are often absent.
There was a lot of variation between subregions and countries, even within countries, and also across the 5 different assessment themes. There was a range in terms of quality from the perfectly acceptable to the downright awful, so the reports present a complicated picture. But, ultimately, we can see that every country has work to do to improve their system of institutional care for mental health while simultaneously pushing to relocate the system of care and support out of these institutions.
Now that we have these data and better understand the scope of the problem, what can and should countries do to change their institutions?
If we want to improve institutional care, we can’t simply renovate or update buildings. The change has to come from inside. Most importantly, we need to build up awareness, skills and literacy around mental health and human rights. This needs to happen at all levels of society, from policy-makers to the actual staff working in institutions. Armed with this knowledge, we can then start to implement more humane practices and give people more positive experiences within – or, far preferably, outside – institutions.
This idea actually takes us to the next phase of work, where we have moved from assessment to quality improvement. For example, next month we are bringing together 15 country teams for advanced QualityRights training with a view to subsequently roll out better standards in selected institutions from each country.
An independent monitoring mechanism is also an important part of raising standards in countries, and WHO recommends that countries give full consideration to the creation of such a mechanism.
Can this kind of change from within help transform mental health care in the long term?
The ultimate goal is to move away from institutionalization and towards community-based care. But that process can be lengthy and requires transitional funding, as we’ve seen in countries that have done it. This report focuses on what we can do right now to improve our human resources, and this does not require a lot of money. It requires us to equip those already working in the system to change their mindset, to see that the people living in institutional care have rights – they need more than just treatment, they need to be treated like individuals with interests and preferences and needs like any of us. Once you start doing this, you begin to understand that long-term institutions really aren’t the right places for these people, and that process will also help move countries towards better models of care.